This Nutrition Connection CE article appeared in the December 2025 issue of Nutrition & Foodservice Edge Express. To view a PDF of this article click HERE.
To earn 1.0 GEN CE credit, purchase the CE article in the ANFP Marketplace HERE or click the button below and complete the quiz.
![]()
This course is a level II continuing competence. View continuing competence level descriptions HERE.

Hidden Hunger in the Elderly: A Focus on Micronutrients
By: Kathy Murdock, MS, RD, LD
DURING LUNCH ON A BUSY DAY IN THE DINING ROOM, Mrs. Jones slowly pushes her tray away. She tells the dietary aide she feels too tired today to eat. Sarah, the dietary manager, notices she has eaten only mashed potatoes and pudding for several meals. Her once lively conversation has faded, and she now requires assistance in daily activities. In addition, nursing staff report increased forgetfulness and unsteadiness over the past week.
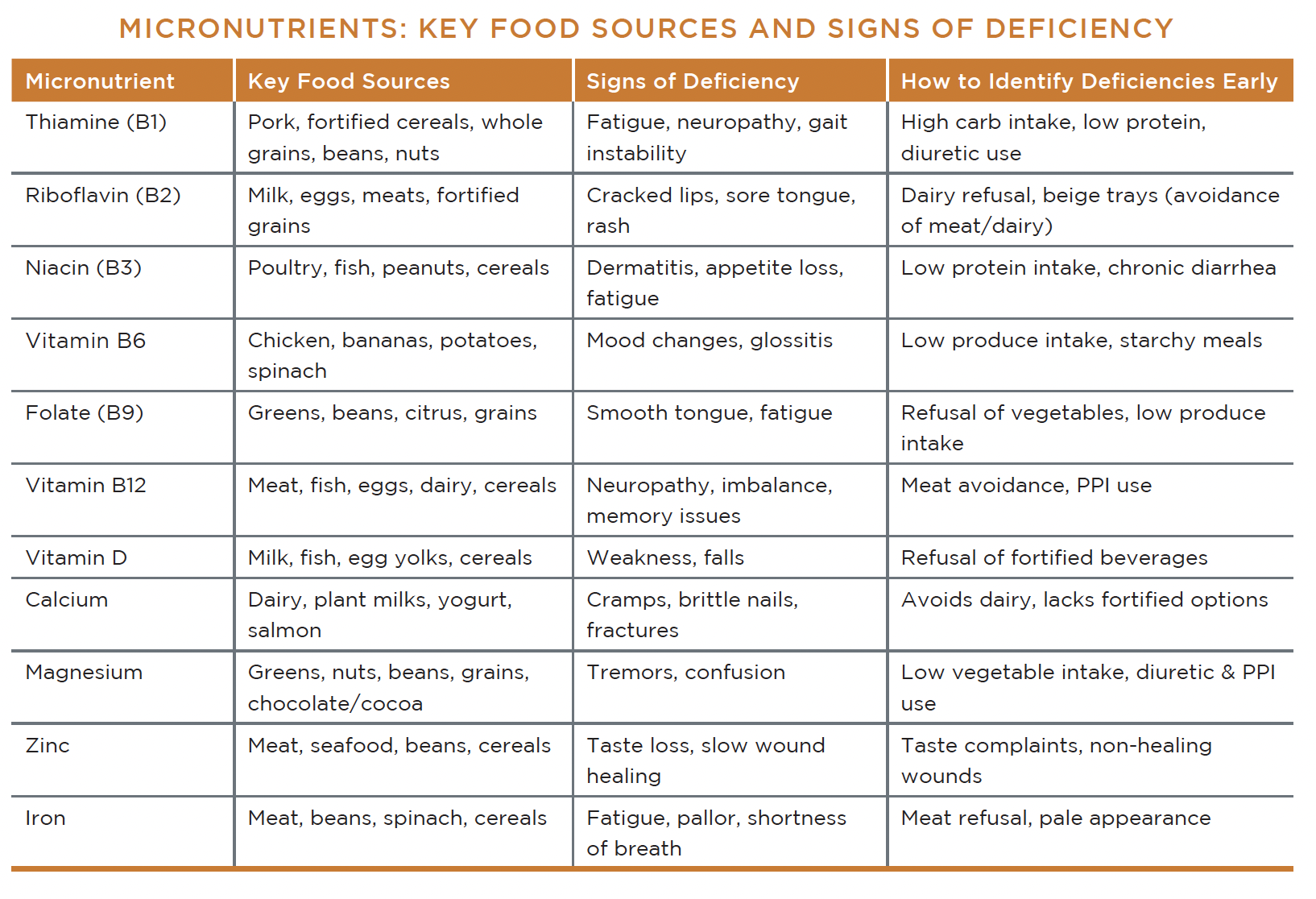
While these symptoms may appear to be part of normal aging, they often signal early micronutrient deficiencies. Fatigue, neuropathy, cognitive issues, muscle weakness, and appetite decline frequently indicate poor intake of thiamine, vitamin B12, iron, vitamin D, or multiple nutrients at once. Many specific micronutrients are commonly deficient in the elderly.
Food-based strategies can improve intakes, and working together as a team to address deficiencies can help with early interventions.
VITAMIN B1 (THIAMINE)
Thiamine, also known as vitamin B1, is essential for converting carbohydrates into usable energy and supporting normal nerve conduction. Older adults often eat soft, carbohydrate-rich foods such as mashed potatoes, baked goods, cereals, and sweetened beverages, which significantly increase carbohydrate intake without contributing adequate thiamine. Diuretics commonly used for heart failure or swelling increase urinary thiamine loss. Residents with chronic low intake or poor appetite can become deficient quickly.
Symptoms often develop slowly, including fatigue, irritability, low motivation, neuropathy, slowed reflexes, and unsteady gait. CDM, CFPPs may observe reduced walking speed when entering or exiting the dining room, or notice residents avoiding protein-rich foods.
To combat deficiency, CDM, CFPPs can encourage consumption of thiamine-rich foods such as fortified cereals, legumes, and pork. Replacing sugary drinks with fortified alternatives and encouraging balanced plates that include protein help stabilize energy and improve intake. Some examples of fortified drinks are milkshakes, fortified juices, and yogurt smoothies.
VITAMIN B2 (RIBOFLAVIN)
Riboflavin (vitamin B2) supports energy production and tissue integrity. Many older adults avoid dairy due to intolerances — whether real or perceived — or preference changes, making riboflavin deficiency more likely. Residents consuming mostly white bread, tea, and desserts receive little to no riboflavin.
Classic signs of deficiency include cracked mouth corners, sore or swollen tongue, facial rash, or inflammation around the nose. CDM, CFPPs may notice residents complaining that certain foods burn or irritate their mouths.
To support riboflavin intake, nutrition professionals can encourage dairy in soft forms such as yogurt, pudding, smoothies, blended soups, and fortified milk. For residents who avoid dairy, sources also include eggs, almonds, mushrooms, and fortified grains. Although many older adults may be lactose intolerant, there are lactose-free dairy alternatives to include in the menu offerings to help avoid inadequate intakes. Many older adults favor homemade shakes over commercial supplements, and food first strategies are preferred.
VITAMIN B3 (NIACIN)
Niacin (vitamin B3) plays a major role in cellular energy production and DNA repair. Chronic diarrhea, low protein intake, or alcohol use increase deficiency risk. Symptoms may be nonspecific including reduced appetite, fatigue, irritability, and skin discoloration or rashes.
Persistent selection of low-protein meals such as bread, fruit cups, and desserts is a strong indicator of low niacin intake. Residents who avoid meats due to chewing difficulty are especially at risk.
To support niacin status, CDM, CFPPs can offer moist poultry dishes, soft flaky fish, peanut butter spreads, enriched cereals, and protein shakes. Adding flavorful sauces or gravies can help residents accept more protein foods, along with assuring that the proper texture consistencies are provided if needed.
VITAMIN B6 (PYRIDOXINE)
Pyridoxine, better known as vitamin B6, plays a major role in neurotransmitter production, red blood cell formation, and immune system function. Older adults absorb B6 less efficiently. Use of soft diets is common in long-term care due to poor dentition or issues with swallowing. Soft diets often limit food variety and might be lower in B6.
Symptoms may include mood instability, irritability, depression-like behavior, glossitis, or mouth soreness. Residents might also show increased infections or slow healing, as B6 affects immune pathways.
To improve intake, CDM, CFPPs can incorporate potatoes, bananas, spinach, chicken, and tuna or other fish into menus. Offering vegetable soups or adding diced vegetables into soft casseroles improves nutrient density without overwhelming residents.
FOLATE (VITAMIN B9)
Folate (vitamin B9) is required for red blood cell formation, DNA synthesis, and cognitive well-being. Residents who consume limited fruits, vegetables, or legumes are most at risk. “Tea-and-toast” diets or diets that lack variety contribute significantly to deficiency.
Symptoms include smooth or swollen tongue, fatigue, irritability, and anemia. Residents may appear disengaged or sleepy following meals.
To increase folate intake, CDM, CFPPs can incorporate tender cooked greens, beans, lentil stews, citrus cups, and fortified grains and cereals. For residents with chewing difficulties, pureed vegetable blends can be stirred into eggs or soups, and fruit can be blended and added to oatmeal, pudding, yogurt, or ice cream.
VITAMIN B12
Vitamin B12 deficiency is extremely common in long-term care due to reduced stomach acid, gastric atrophy, and medications such as PPIs or Metformin. Soft diets may reduce meat consumption, further increasing the risk of deficiency.
B12 deficiency signs can include neuropathy, numbness, poor coordination, memory issues, confusion, or increased falls. These symptoms mimic dementia and often go unnoticed unless changes are reported to the care team.
To help combat this deficiency, CDM, CFPPs can offer fortified cereals, dairy products, scrambled eggs, yogurt parfaits, and tender meats. Residents with limited intake may benefit rom fortified nutritional beverages recommended by the dietitian.
VITAMIN D
Vitamin D supports muscle strength, immunity, and fall prevention. Older adults receive limited sun exposure, vitamin D absorption through the skin decreases with age, and few foods naturally contain vitamin D. These issues are the reason vitamin D deficiency is very common among older adults.
Symptoms include muscle weakness, bone pain, fatigue, or frequent falls. Residents with a history of fractures or low mobility are particularly vulnerable.
CDM, CFPPs can promote intake of fortified milk, cereals, egg yolks, or fish. Coordination with the dietitian is essential, as supplementation is often required to achieve adequate levels.
CALCIUM
Calcium is essential for bone density, muscle contraction, and nerve transmission. As explained earlier, many older adults avoid dairy, making deficiencies very common in this population. Determining true intolerances by communicating with the resident, the dietitian, and the care team can help increase intake of calcium. Many times, a lactose-free alternative can be provided with good acceptance after proper counseling with the resident.
Signs of deficiency include muscle cramps, brittle nails, tingling sensations, and increased fracture risk. Residents who have a deficiency may complain of leg cramps.
To strengthen calcium intake, CDM, CFPPs can offer yogurt, cottage cheese, fortified plant milks, powdered milk added to mashed potatoes, and blended dairy drinks. Being creative with recipes for snacks that are calcium-rich can also help increase intake of calcium. Some examples are yogurt parfaits and smoothies. Remember to add garnishes that are allowed on the diet to increase visual appeal.
MAGNESIUM
Magnesium deficiency is common in the elderly, which can be due to decreased intestinal absorption, excessive urinary excretion, or poor dietary intake. Diuretic use, diarrhea, and low vegetable intake are common causes of deficiency. Excessive coffee, soft drink, and processed food consumption can all affect magnesium status.
Magnesium has many important roles in the body including the support of heart rhythm, muscle function, and cognitive stability. It also plays a major role in DNA synthesis and energy metabolism. Deficiencies can impact glucose homeostasis, blood pressure, heart health, as well as bone health.
Symptoms of low magnesium levels may include tremors, twitching, confusion, or irritability. Residents may show worsening sleep quality or muscle spasms.
To increase consumption of magnesium in the diet, add cooked leafy greens or pureed vegetables to soft foods such as casseroles or soups, offer bean-based soups, and add whole-grain cereals, shredded nuts, or shaved chocolate to pudding parfaits.
ZINC
Zinc supports taste, appetite regulation, and wound healing. Low zinc results in altered tastes, which further reduces intake, creating a cycle of decline.
Symptoms include prolonged wound healing, loss of taste, hair thinning, and reduced appetite. CDM, CFPPs may notice residents saying food has no flavor.
To improve zinc intake, nutrition professionals can offer beans, ground meats, seafood salads, fortified cereals, and enriched sauces. Soups are a great way to include ingredients and provide comfort foods for residents who aren’t eating meals well. For residents with poor intake, zinc-rich snacks such as pudding with added protein or fortified beverages may also be an effective intervention.
IRON
Iron is needed for oxygen transport, energy, and immune function. Residents who avoid meat or have chronic inflammation frequently develop a deficiency in this micronutrient.
Symptoms include fatigue, pallor, cold intolerance, low energy, and shortness of breath. CDM, CFPPs may notice residents leaving meat uneaten or tiring quickly during meals.
To support iron intake, offer tender meats, meat or bean-based soups, dark leafy greens, fortified cereals, and iron-rich casseroles. Pairing iron-rich foods with vitamin C sources — such as citrus cups — enhances absorption.
STRENGTHENING CDM, CFPP AND RDN COLLABORATION
Preventing and correcting micronutrient deficiencies requires a strong, proactive partnership between CDM, CFPPs and registered dietitian nutritionists (RDNs). CDM, CFPPs observe residents daily, note changes in appetite, and recognize refusal patterns or sensory aversions. They also monitor tray accuracy, meal consistency, and environmental barriers that influence intake.
RDNs contribute clinical interpretation, assess lab values, review medications, and develop treatment strategies including fortified foods, supplements, and individualized nutrition care plans. When CDM, CFPPs and RDNs communicate effectively, possible deficiencies can be identified early and corrected before they lead to serious health declines.
Key areas of collaboration include regular review of high-risk residents, joint participation in care plan meetings and communication with other members of the care team, early reporting of appetite decline, identification of swallowing or chewing concerns, and shared troubleshooting of barriers such as texture limitations or dislike of specific foods.
CDM, CFPPs can also support RDNs by evaluating menu patterns for nutrient density, suggesting recipe or menu adjustments, monitoring staff compliance, and ensuring consistent delivery of supplements or fortified foods. RDNs can provide updated training, nutrient guidelines, and education on best practices for micronutrient monitoring.
Together, this partnership ensures that every resident receives nutrient-dense meals tailored to their needs and has the highest opportunity for improved function, comfort, and quality of life.
SUMMING IT UP
Micronutrient deficiencies often develop gradually and can be mistaken as normal signs of aging. CDM, CFPPs play a crucial role in identifying early changes in appetite, mood, mobility, and intake patterns. In Mrs. Jones’s case, her fatigue, gait instability, and meal refusal patterns suggested possible deficiencies in thiamine, vitamin B12, and iron. By reporting these concerns promptly, the dietitian was able to evaluate her needs, recommend appropriate fortified foods, and coordinate supplementation with the care team. Within weeks, her energy and engagement improved. This demonstrates how early detection and strong collaboration with the entire care team can reverse decline and significantly improve resident well-being. Numerous micronutrient deficiencies are common and can exist at once. CDM, CFPPs can play an important role in residents’ nutritional care by identifying risk factors and communicating with the care team.
About the Author
Kathy Murdock, MS, RD, LD
Kathy Murdock has been working in nutrition and dietetics since 2007. She is currently a consultant dietitian in long-term and acute care in rural southeast Missouri and northeast Arkansas. She has a passion for teaching, writing, and public speaking. Murdock previously worked for a community college in northeast Arkansas teaching future CDM, CFPPs.