This Nutrition Connection CE article appeared in the December 2023 issue of Nutrition & Foodservice Edge Express. To view a PDF of this article click HERE.
To earn 1.0 GEN CE credit, purchase the CE article in the ANFP Marketplace HERE or click the button below and complete the quiz.
![]()
This course is a level I continuing competence. View continuing competence level descriptions HERE.

Team-Based Nutrition Screening, Assessment, and System Management for Successful Outcomes
By: Brenda Richardson, MA, RDN, LD, FAND
AS A CRITICAL COMPONENT OF QUALITY OF LIFE AND CARE, nutrition services continue to need improvement in all healthcare settings. Malnutrition is a problem that is often not identified in hospitals; 8 percent of hospital patients are diagnosed, but malnutrition is estimated to affect 20-50 percent of patients.
Older adults are at greater risk of malnutrition because of higher rates of disease-associated, function-associated, social/mental health-associated, and hunger/food insecurity-associated risk factors as compared to the general population. Those 85 and older have the highest incidence of malnutrition-related hospital stays at 35 times the rate of 18–39-year-olds, and 8.6 times the rate of 40–64-year-olds. Malnutrition in elderly populations is associated with poor clinical outcomes and is an indicator for increased mortality.
It is generally assumed that federal regulations and The Joint Commission requirements are adequate. However, such an assumption is not accurate. The federal Conditions of Participation (CoP) regulations do not specifically address malnutrition. In long-term care nursing facilities, Nutrition/Hydration Maintenance FTag 692 continues to be in the top 25 deficiencies in the U.S. for nursing facilities, however these FTags may not always be accurate indicators of malnutrition.
The Joint Commission is an independent, not-for-profit accreditation body that sets standards in health care and accredits over 22,000 healthcare organizations. Accreditation by The Joint Commission is voluntary, but passing an accreditation survey (about once every 36 months) indicates a hospital meets the federal regulations necessary to receive payment from Medicare and Medicaid programs. Although The Joint Commission requires that hospitals screen for risk of malnutrition as part of the general admission process, hospital practices vary.
Healthcare facilities with effective nutritional programs and positive outcomes integrate practice around basic principles. This article highlights two principles to help healthcare facilities improve nutritional care and services for successful outcomes.
PRINCIPLE #1: NUTRITION SCREENING AND ASSESSMENT REQUIRE A TEAM
Malnutrition is defined as an acute, subacute, or chronic state of nutrition in which a combination of varying degrees of overnutrition or undernutrition with or without inflammatory activity have led to a change in body composition and diminished function.
Evaluation of nutritional status is critical, either to identify if an individual has nutritional imbalance due to an underlying condition, or to assess if an individual is likely to develop a medical condition due to nutritional imbalance. A detailed, systematic evaluation of nutritional status conducted by a team of healthcare providers to diagnose malnutrition and then guide the interventions embodies the complete nutritional care process.
Hence, a comprehensive evaluation of a patient’s nutritional status is warranted. A comprehensive nutritional assessment, however, should be differentiated from nutritional screening. Nutritional screening is done to quickly identify individuals at risk of developing malnutrition. Here’s a more detailed look at the distinctions:
Nutrition screening is the process of identifying patients, clients, or groups who may have a nutrition diagnosis and benefit from nutrition assessment and intervention by a registered dietitian (RD) or registered dietitian nutritionist (RDN). During the screening process, it is crucial to not miss individuals with potential risk for nutrition problems. Otherwise, the patient is not referred to an RDN for nutrition assessment to determine need for nutrition intervention. A positive screen for malnutrition risk enables access to nutrition care for malnourished individuals who need it.
Nutrition Screening Components:
- Nutrition screening may be conducted in any practice setting as appropriate.
- Nutrition screening tools should be quick, easy to use, valid, and reliable for the patient, population, and setting.
- The nutrition screening process and parameters are established for the institution by a multidisciplinary team (including RDNs).
For example, the mini nutritional assessment (MNA) is a commonly-used tool utilized in the geriatric patient population to screen for individuals at risk of malnutrition. This screening tool consists of a questionnaire and has a scoring system that helps identify at-risk individuals. A comprehensive nutritional assessment is then performed to evaluate the nutritional status of patients already identified at nutritional risk.
Nutritional assessment allows healthcare providers to systematically assess the overall nutritional status of patients, diagnose malnutrition, identify the underlying nature of disease(s) that lead to malnutrition, and plan necessary interventions.
While performing nutritional assessment, it is important to understand that there is no single best test to evaluate nutritional status. Information should be collected systematically, and an evaluation of nutritional status should be done based on the overall data collected. As per the American Society for Parenteral and Enteral Nutrition (ASPEN) guidelines, a comprehensive nutritional assessment involves a thorough clinical examination (history and physical exam), anthropometric measurements, diagnostic tests, and dietary assessments.
Team-based nutrition evaluation, from a clinical standpoint, helps detect malnutrition or factors causing it early, which allows for early intervention and better clinical outcomes. This requires the involvement of physicians (generalists and specialty care physicians); nurses; registered dietitian nutritionists (RDNs); nutrition and dietetics technicians, registered (NDTRs); certified dietary manager, certified food protection professionals (CDM, CFPPs); pharmacists; dentists; and laboratory personnel. The primary attending physician is responsible for overall patient care. Since nutritional status is an important predictor of healthcare outcomes, nutritional assessment and intervention by the primary attending physician is critical.
The RDN, NDTR, and CDM, CFPP play vital roles in the overall nutritional evaluation. For example, NDTRs and CDM, CFPPs are qualified to assist with general nutrition screenings and may also assist dietitians and other members of the healthcare team with identifying patients at risk for malnutrition in the clinical setting. RDNs are trained to perform medical nutrition therapy (MNT) using the Nutrition Care Process (NCP), which includes nutrition assessment as the first step in identifying potential nutrition problems in patients, such as the risk factors of malnutrition.
The five domains of nutrition assessment outlined in the NCP include:
- Food or nutrition-related history
- Biochemical data, medical tests, and procedures
- Anthropometric measurements
- Nutrition-focused physical findings
- Client history
Scope of practice in nutrition and dietetics encompasses the range of roles, activities, laws, and regulations within which nutrition and dietetics practitioners perform. For credentialed practitioners, scope of practice is typically established within the practice act, and is interpreted and controlled by the agency or board that regulates the practice of the profession in each state.
Scope of Practice and Professional Standards of Practice for RDNs and NDTRs are established by the Academy of Nutrition and Dietetics.
Scope of Practice and Professional Standards of Practice for CDM, CFPPs are established by the Certifying Board for Dietary Managers, as the credentialing agency for the Association of Nutrition & Foodservice Professionals.
Certified dietary manager, certified food protection professionals (CDM, CFPPs) play an important role in nutrition evaluation. The CDM, CFPP is qualified to perform the tasks within the Nutrition domain as seen in the figure below.
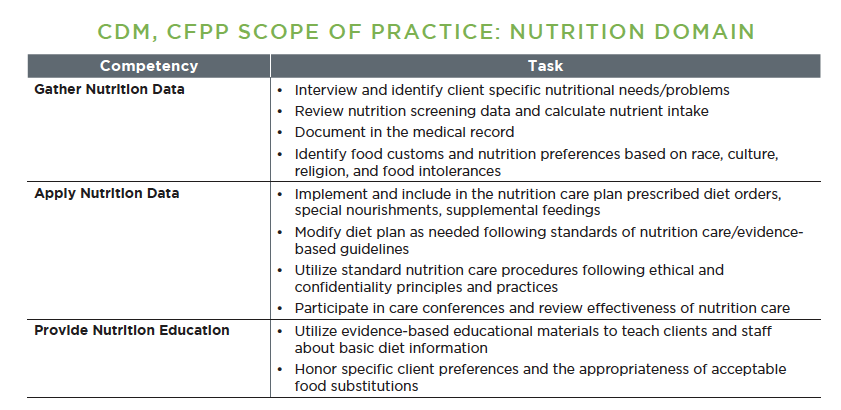
Professional Standards of Practice serve as the basis for quality dietetic practice for CDM, CFPPs. The standards that follow provide guidelines for certified dietary manager, certified food protection professionals to use when documenting food and fluid intake in the medical record.
Standard 1: The Certified Dietary Manager, Certified Food Protection Professional (CDM®, CFPP®) shall ensure that nutritional screening data is accurately obtained and recorded in the medical record in accordance with state and federal regulations and facility policy. The CDM, CFPP shall ensure that food and fluid-related interventions are added to client care plans.
Standard 2: The Certified Dietary Manager, Certified Food Protection Professional (CDM, CFPP) shall ensure that procedures for documenting nutritional assessment are established according to regulatory agency guidelines and facility policy.
For the CDM, CFPP participating in collaborative dietetics, practice standards serve as guidance for documenting in the medical record. Reference to the standards aids in development of facility policies regarding nutritional screening and assessment of clients.
Nurses also help with early nutritional screening to identify nutrition risk factors and monitor the patient’s condition to maintain timely documentation records of clinical status. Pharmacists may provide information about potential drug side effects, drug-nutrient interactions, or conditions that may impact the risk of malnutrition.
Dental professionals can play a unique role in identifying malnutrition risk factors in patients. Other healthcare team members’ services and expert opinions are also essential based on a patient’s clinical presentation.
Collaboration between each healthcare team member working within their Scope of Practice and Professional Standards of Practice is essential to provide effective, comprehensive nutritional care and services.
PRINCIPLE #2: EFFECTIVE NUTRITION SYSTEMS AND PROCESSES REQUIRE A TEAM
Overall, effective collaboration between each healthcare team member is essential to provide thorough, comprehensive nutritional care and services. Interdisciplinary teamwork is critical in all nutrition-related programs and services such as:
- Medical record documentation
- Nutrition at risk
- Hydration
- Supplements
- Weight
- Dining/meals/snacks
- Skin/wound care
- Behavior management
- Continuous quality improvement
CONCLUSION
As this article highlights, there are many different components of nutritional care and services, and it would be impossible for one member or department of the healthcare team to assume responsibility for all components alone. While federal regulations and The Joint Commission requirements assist in some aspects of nutrition services, it is effective team-based nutritional screening, assessment, and interventions that will break the vicious cycle between malnutrition and various diseases or conditions.
About the Author
Brenda Richardson, MA, RDN, LD, FAND
Brenda Richardson is a lecturer, author, and owner/president of Brenda Richardson, LLC. She is a long-time RDN consultant in long-term care, and also serves as an Independent Auditor for the Gluten-Free Certification Organization.