This Nutrition Connection CE article appeared in the 2024 Sept/Oct issue of Nutrition & Foodservice Edge magazine. To view a PDF of this article click HERE.
To earn 1.0 GEN CE credit, purchase the CE article in the ANFP Marketplace HERE or click the button below and complete the quiz.
![]()
This course is a level I continuing competence. View continuing competence level descriptions HERE.

Revisiting the RAI Process for Nutrition
By: Brenda Richardson, MA, RDN, LD, FAND
FOR HEALTHCARE PROFESSIONALS working in long-term care (LTC), it is important to understand the Resident Assessment Instrument (RAI) process. Nutrition is embedded throughout this process, and it is vital to know how to address nutrition for success with quality, regulatory, and financial outcomes.
This article is based on the draft Minimum Data Set (MDS) 3.0 Resident Assessment Instrument (RAI) Manual released in June 2024 with revisions that become effective October 1, 2024. The manual has more than 900 pages. This article will review important basics of the process to explain how the components work together.
OVERVIEW OF THE RESIDENT ASSESSMENT PROCESS
The RAI helps nursing home staff gather definitive information on a resident’s strengths and needs, which must be addressed in an individualized care plan. It also assists staff with evaluating goal achievement and revising care plans accordingly by enabling the nursing home to track changes in the resident’s status. As the process of problem identification is integrated with sound clinical interventions, the care plan becomes each resident’s unique path toward achieving or maintaining their highest practical level of well-being.
The RAI helps the staff look at residents holistically—as individuals for whom quality of life and quality of care are mutually significant and necessary. Interdisciplinary use of the RAI promotes this emphasis on quality of care and quality of life. Involving disciplines such as dietary, social work, physical therapy, occupational therapy, speech-language pathology, pharmacy, and activities/recreational therapy in the RAI process has fostered a more holistic approach to resident care and strengthens team communication. This interdisciplinary process also helps to support the spheres of influence on the resident’s experience of care, including workplace practices, the nursing home’s cultural and physical environment, staff satisfaction, clinical and care practice delivery, shared leadership, family and community relationships, and federal/state/local government regulations.
It is important to read the RAI Manual, as it is the primary source of information for completing an MDS assessment, and using it correctly increases the accuracy of assessments. Be sure to understand and apply information in Chapter 3 for proper MDS coding, and be familiar with Chapters 1, 2, 4, 5, as these chapters provide the framework and supporting information for data collected on the item set as well as the process for further assessment and care planning, submitting and modifying assessments, and information on the SNF Prospective Payment System (PPS). The actual manual with in-depth explanations can be found on the CMS website: CMS MDS 3.0 RAI Manual
CONTENT OF THE RAI FOR NURSING HOMES
The RAI consists of three basic components. Utilization of the three components of the RAI yields information about a resident’s functional status, strengths, weaknesses, and preferences, as well as offers guidance on further assessment once problems have been identified. Each component flows naturally into the next as follows:
- Minimum Data Set (MDS). This core set of screening, clinical, and functional status data elements, including common definitions and coding categories, forms the foundation of a comprehensive assessment for all residents of nursing homes certified to participate in Medicare or Medicaid.
- Care Area Assessment (CAA) Process. This process is designed to assist the assessor to systematically interpret the information recorded on the MDS. Once a care area has been identified or “triggered,” nursing home providers use current, evidence-based clinical resources to conduct an assessment of the potential problem and determine whether or not to care plan for it. Specific components of the CAA process include:
- Care Area Triggers (CATs) are specific coding responses for one or a combination of MDS data elements. The triggers identify residents who have, or are at risk for developing, specific problems and require further assessment.
- Care Area Assessment is the further investigation of triggered areas, to determine if the care area triggers require interventions and care planning.
- CAA Summary (Section V of the MDS 3.0) provides a location for documentation of the care area(s) that have triggered from the MDS, and the decisions made during the CAA process regarding whether or not to proceed to care planning.
- Utilization Guidelines. Also known as the Long-Term Care Facility Resident Assessment Instrument 3.0 User’s Manual, this includes instructions for completion of the RAI as well as structured frameworks for synthesizing MDS and other clinical information.
Over time, the various uses of the MDS have expanded. The primary purpose as an assessment instrument is to identify resident care problems that are addressed in an individualized care plan, and data collected from MDS assessments is used for the Skilled Nursing Facility Prospective Payment System (SNF PPS) Medicare reimbursement system, many State Medicaid reimbursement systems, and monitoring the quality of care provided to nursing home residents. The MDS has also been adapted for use by non-critical access hospitals (non-CAHs) with a swing bed (SB) agreement. Non-CAH SBs are required to complete the MDS for reimbursement under the SNF PPS.
The RAI process also has multiple regulatory requirements including:
- The assessment accurately reflects the resident’s status.
- A registered nurse conducts or coordinates each assessment with the appropriate participation of health professionals.
- The assessment process includes direct observation, as well as communication with the resident and direct care staff on all shifts.
Nursing homes are responsible for determining who should participate in the assessment process, how the process is completed, and how the assessment information is documented while remaining in compliance with the requirements of the federal regulations and the instructions contained within the manual.
The pathway diagram above illustrates a problem identification process flowing from MDS (and other assessments) to the CAA decision-making process, care plan development, care plan implementation, and finally to evaluation.
Regulations require nursing homes that are Medicare certified, Medicaid certified or both, to conduct initial and periodic assessments for all their residents. The Resident Assessment Instrument (RAI) process is the basis for the accurate assessment of each resident.
Chapter 3 of the RAI Manual provides item-by-item coding instructions for all required sections and items in the MDS Version 3.0 item sets, and the most common section of the MDS used for Nutrition is Section K: Swallowing/Nutritional Status.
The intent of Section K is to assess the many conditions that could affect the resident’s ability to maintain adequate nutrition and hydration. This section covers swallowing disorders, height and weight, weight loss, and nutritional approaches. The assessor should collaborate with the dietitian and dietary staff to ensure that items in this section have been assessed and calculated accurately.
Planning for Care with Section K should include provisions for monitoring the resident during mealtimes and during functions/activities that include the consumption of food and liquids. When necessary, the resident should be evaluated by the physician, speech-language pathologist, and/or occupational therapist to assess for any need for swallowing therapy and/or to provide recommendations regarding the consistency of food and liquids.
Section K assesses for signs and symptoms that suggest a swallowing disorder that has not been successfully treated or managed with diet modifications or other interventions (e.g., tube feeding, double swallow, turning head to swallow, etc.), and therefore represents a functional problem for the resident.
THE RESIDENT ASSESSMENT INSTRUMENT (RAI) AND CARE AREA ASSESSMENTS (CAAS)
In accordance with regulations, the facility must develop a comprehensive care plan for each resident that includes measurable objectives and timetables to meet a resident’s medical, nursing, and mental and psychosocial needs that are identified in the comprehensive assessment. The care plan should outline services that are to be furnished to attain
or maintain the resident’s highest practicable physical, mental, and psychosocial well-being, and any services that would otherwise be required but are not provided due to the resident’s exercise of rights, including the right to refuse treatment.
The completed MDS must be analyzed and combined with other relevant information to develop an individualized care plan. To help nursing facilities apply assessment data collected on the MDS, Care Area Assessments (CAAs) are triggered responses to items coded on the
MDS specific to a resident’s possible problems, needs, or strengths.
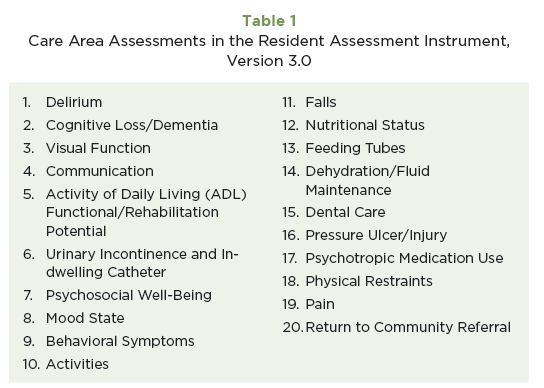
Specific Care Area Triggers (CATs) logic for each care area is identified under 20 Care Areas (see Table 1). The CAAs reflect conditions, symptoms, and other areas of concern that are common in nursing home residents and are often identified or suggested by MDS findings. Interpreting and addressing the care areas identified by the CATs is the basis of the Care Area Assessment process and can help provide additional information for the development of an individualized care plan.
The CAA process does not mandate any specific tool for completing the further assessment of the triggered areas, nor does it provide any specific guidance on how to understand or interpret the triggered areas. Instead, facilities are instructed to identify and use tools that are current and grounded in current clinical standards of practice, such as evidence-based or expert-endorsed research, clinical practice guidelines, and resources.
OTHER CONSIDERATIONS REGARDING USE OF THE CAAS
- Assigned responsibility for completion: Per the OBRA statute, the resident’s assessment must be conducted or coordinated by a registered nurse (RN) with the appropriate participation of health professionals. It is common practice for facilities to assign specific MDS items or portion(s) of items (and subsequently CAAs associated with those items) to those of various disciplines (e.g., the dietitian completes the Nutritional Status and Feeding Tube CAAs, if triggered). The proper assessment and management of CAAs that are triggered for a given resident may involve aspects of diagnosis and treatment selection that exceed the scope of training or practice of any one discipline involved in the care (for example, identifying specific medical conditions or medication side effects that cause anorexia leading to a resident’s weight loss). It is the facility’s responsibility to obtain the input that is needed for clinical decision-making (e.g., identifying causes and selecting interventions) that is consistent with relevant clinical standards of practice.
- The facility should be able to provide surveyors with their chosen protocols and resources selected that they have used upon request as part of the survey review process.
Written documentation of the CAA findings and decision-making process may appear anywhere in a resident’s record; for example, in discipline-specific flow sheets, progress notes, the care plan summary notes, a CAA summary narrative, etc. Nursing homes should use a format that provides the information as outlined in the RAI Manual and the State Operations Manual (SOM). If it is not clear that a facility’s documentation provides this information, surveyors may ask facility staff to supply such evidence.
The “Location and Date of CAA Documentation” column on the CAA Summary (Section V of the MDS 3.0) is used to identify where the CAA information and decision-making documentation can be found in the resident’s record, and to indicate in the column “Care Planning Decision” whether the triggered care area is addressed in the care plan. Access Section V by scanning the QR code provided above.
Appendix C of CMS’s RAI Version 3.0 Manual contains both specific and general resources that may be chosen to further assess care areas triggered from the MDS 3.0 Resident Assessment Instrument (RAI). CMS resources are provided in this appendix solely as a courtesy in completing the RAI CAA process. CMS does not mandate, or endorse the use of any resource, including those provided in this appendix. However, nursing homes should ensure that the resource(s) they use are current, evidence-based, or expert-endorsed research and clinical practice guidelines/resources.
Appendix C of the RAI Version 3.0 Manual for #12 Nutritional Status Care Area (Review of Indicators of Nutritional Status) can be found in the QR code provided above.
Other common CAAs used with nutritional care include #13: Feeding Tubes and #14: Dehydration.
CONCLUSION
The intent of this article is to offer an overview of the Resident Assessment Instrument process and resources to assist healthcare professionals in providing effective, quality nutritional care and services. For healthcare professionals working in long-term care, it is important to understand the RAI process. Nutrition is embedded throughout this process and should be a collaborative effort between the Registered Dietitian; Certified Dietary Manager, Certified Food Protection Professional; and other members of the nutrition team for success with quality, regulatory, and financial outcomes.
About the Author
Brenda Richardson, MA, RDN, LD, FAND
Brenda Richardson is a lecturer, author, and owner/president of Brenda Richardson, LLC. She is a long-time RDN consultant in long-term care, and also serves as an Independent Auditor for the Gluten-Free Certification Organization.