April 30, 2024
This Nutrition Connection CE article appeared in the 2024 March/April issue of Nutrition & Foodservice Edge magazine. To view a PDF of this article click HERE.
To earn 1.0 GEN CE credit, purchase the CE article in the ANFP Marketplace HERE or click the button below and complete the quiz.
![]()
This course is a level I continuing competence. View continuing competence level descriptions HERE.

The Brain Science Behind Comfort Foods
By: Kristin Klinefelter, MS, RDN, LDN
“AS I ALWAYS SAY, NO GUTS, NO DIGESTION!” says Mrs. Frizzle and off they go! The lucky children that ride the Magic School Bus (Cole 1990) with their eccentric and brilliant teacher are learning about the digestive system today. Oh, the adventures they go on, learning about their bodies and health.
I often try to channel my inner Mrs. Frizzle while teaching young people about how their digestive system works. Actually, even my adult learners in clinic or education benefit from descriptions of HDL cholesterol acting like a dump truck, picking up the LDL as it “drives” around our blood system. I have a very clinical-looking digestive system poster hanging on the wall, but make sure I have stickers that are fun and located in key areas along the system to bring a simple level of understanding for all people to relate to.
In whatever area of nutrition and food service you work, you must have a good understanding of our digestive system: how absorption works, which organs are affected by diseases, and foods and diets that are necessary to treat those diseases. Let’s do a deep dive into the top diseases and how they affect the digestive system, and hopefully have a little fun while we travel through the gastrointestinal (GI) tract. We will follow the path of a simple lunch being digested and absorbed.
Today’s Menu: Grilled Chicken Sandwich with Whole Grain Bun, Lettuce, Tomato & Mayonnaise, Apple Slices, Carrots and Ranch Dip, Chocolate Chip Cookie and 1% Milk. Note: we will mostly talk about what happens to the macronutrients, not the micronutrients on this ride. Let’s go!
First stop, the mouth. Bites of the chicken sandwich and sides are chewed with teeth in the process called mastication, which is mechanical digestion. Immediately upon first bite—or even before—the salivary glands begin to secrete salivary amylase and enact the chemical digestive function of the mouth. Salivary amylase begins digesting the carbohydrate in our lunch (the bun). The mouth does a lot of work chewing and forming a bolus of food to be safely swallowed. Thankfully, our brain and taste buds are just enjoying the lunch and do not have to tell our digestive system to prepare for what is to come!
Digestive and nutrition problems can begin in the mouth. A few disease states cause xerostomia or “dry mouth.” It also can be caused by aging and certain medications. Some key culprits are anticholinergics (to treat incontinence), antidepressants, stimulants, opioids, benzodiazepines (to treat anxiety, insomnia, and other conditions), and antipsychotics (Wang 2018). If you work in long-term care, most likely your aging clients are prescribed at least one of these medications.
Now enter problems that can be related to the mechanical function of the mouth…dental issues. Whether a person has poor dentition, multiple caries, unhealthy gums, or no teeth, dental concerns are the first nutrition problem of the GI system. You likely know plenty of hearty people who overcome their dental problems by modifying their chewing; however, it is our job to provide meals that the client can safely and effectively eat. This is why we have texture-modified diets and speech therapists! Adherence to modified consistency diets for chewing (and swallowing) problems is the key nutrition therapy for our folks with dental problems.
The next critical step to digestion is proper swallowing. Swallowing involves first the tongue pushing the bolus back towards the back of the oral cavity, or the pharynx. Next, there is an action that pushes it into the esophagus. The epiglottis, the cartilage “flap” over the entrance to the trachea, prevents the bolus of food from entering the trachea and causing aspiration into the lungs. With aging, the function of the epiglottis can diminish, increasing risk for aspiration. When the bolus makes it to the esophagus, the digestive function is purely mechanical, as peristalsis moves it down to the entrance of the stomach. Enjoy the ride, chicken sandwich lunch!
Disease states that affect the esophagus include gastroesophageal reflux (GERD), dysphagia, and cancer. A person with oral or esophageal cancer may need long-term tube feeding therapy, as they are not able to consume food or fluids by mouth and esophagus after surgery or chemotherapy. Nutrition therapy for dysphagia involves deep understanding and implementation of the IDDSI framework, which provides a consistent continuum of food and fluid levels. If you have not done so already, learn more about the International Dysphagia Diet Standardisation Initiative (IDDSI) and how to implement it in your facility.
After the brief trip down the esophagus, your bolus will enter the stomach for storage, and protein digestion soon begins. Our chicken is starting to combine with the enzyme pepsin and hydrochloric acid to form chyme (chemical digestion). The stomach also churns (mechanical digestion) at this stage, moving the chyme down into the small intestine. It is important to note that the chicken (protein) and mayo & dressing (fat) stay in the stomach the longest, as the bun (carbohydrate) digestion has already begun in the mouth. The fibers in the carrots, tomato, lettuce, and apple are still moving down the tract.
Disease states that can impact the digestive function of the stomach include gastroparesis (delayed gastric emptying sometimes caused by uncontrolled diabetes), stomach ulcers, food intolerances, and irritable bowel syndrome (IBS) to name just a few. Nutrition therapy and therapeutic diets for the aforementioned disease states are to be individualized and consistent. You have probably witnessed an anxious person with IBS eating a meal in public worried about the food causing them an emergency trip to the restroom. It is an important part of our job to provide foods that will not trigger their bowel problems, even if they do not have a diet order related to it. Thankfully, with the evolution of culture change due to CMS mandates, we have liberalized and simplified our diet orders, but our clients’ nutrition habits have become more sophisticated. Knowing and honoring each one of their diet preferences is an important task! If your client has gastroparesis, or delayed gastric emptying, offer small meals more often that are low-fat and low-fiber (Zikmund). Your client may also be on digestive enzymes, insulin, or certain medications that will take effect by the time the food enters the stomach, so meal and medication timing is critical.
Accessory organs including the liver, pancreas, and gallbladder are important team members of the GI system. When our lunch makes it to the stomach and leaves to the small intestine, the pancreas gets a phone call to release insulin to assist the glucose into our cells. Let’s say we skipped this delicious lunch and our body needed some energy. In this case, our liver gets a call to release glycogen. The pancreas also releases enzymes and other hormones necessary for metabolic processes. Diseases in these accessory organs include gallbladder disease (or no gallbladder after a cholecystectomy), pancreatitis, type 1 diabetes, cirrhosis of the liver, and fatty liver. Nutrition therapy is critical and individualized for these disease states.
By the time your food leaves the stomach, your macronutrients (carbohydrate, protein, fat) have been broken down into elemental (tiny) components of glucose, amino acids, and lipids. Vitamins, minerals, and water continue on down the line as well into the small intestine.
The small intestine measures in at a whopping 22 feet long (Zikmund). In my community college nutrition class, a favorite lesson is ‘building the GI tract.’ The small intestine group gets to cut a thick piece of fuzzy yarn and show how long it is. The class is amazed that it spans the entire classroom! The inner lining of the small intestine has fingerlike projections called villi. This is when I encourage people to hold up their hands, turn their fingers towards each other, and wiggle them around. Those wiggly fingers are like the villi, “sucking” the tiny nutrients into the bloodstream for absorption. A disease state that affects these villi is celiac disease, an autoimmune disorder that attacks these cells, preventing the person from properly absorbing the proteins in gluten. The results include a variety of symptoms such as fatigue, malnutrition, bloating, gas, and diarrhea. The only treatment for celiac disease is diet (Posner, 2019). The person must completely avoid gluten exposure. In the early stages, before those villi have a chance to regenerate, they may also need to avoid lactose. Other disease states that affect the small intestine include Crohn’s disease, colitis, and cancer.
After the 22-foot journey through the small intestine, the fibers in your lunch (the fibers in your apple, lettuce, tomato seeds, carrots) finally make it to the large intestine. Fiber is the “last one standing” of the nutrients, as the human digestive system cannot break it down into glucose for energy. This is why we encourage people to increase insoluble fiber for improved bowel health (Zikmund). The large intestine is 5-feet of smooth tissue that pulls water in to form feces and remove waste. Problems in the large intestine can include fecal impaction, constipation, polyps, diverticulitis, Crohn’s disease, and colorectal cancer.
What comes next is fecal elimination out of the anus. Problems with the anus can include hemorrhoids or fissures. Diets for constipation (high fiber, water) can help prevent these issues, but not treat them (Zikmund). “Pooping problems” can be common talk amongst some of our populations, but other people do not feel as comfortable discussing gas, their bowels, or GI concerns in general. It is important to “normalize potty talk” so we can help the client with basic education and referrals to the registered dietitian nutritionist (RDN). Using resources like the Bristol Stool Chart can assist with these conversations. I often say “oh I talk about poop all day” when someone seems embarrassed to tell me about their GI concerns.
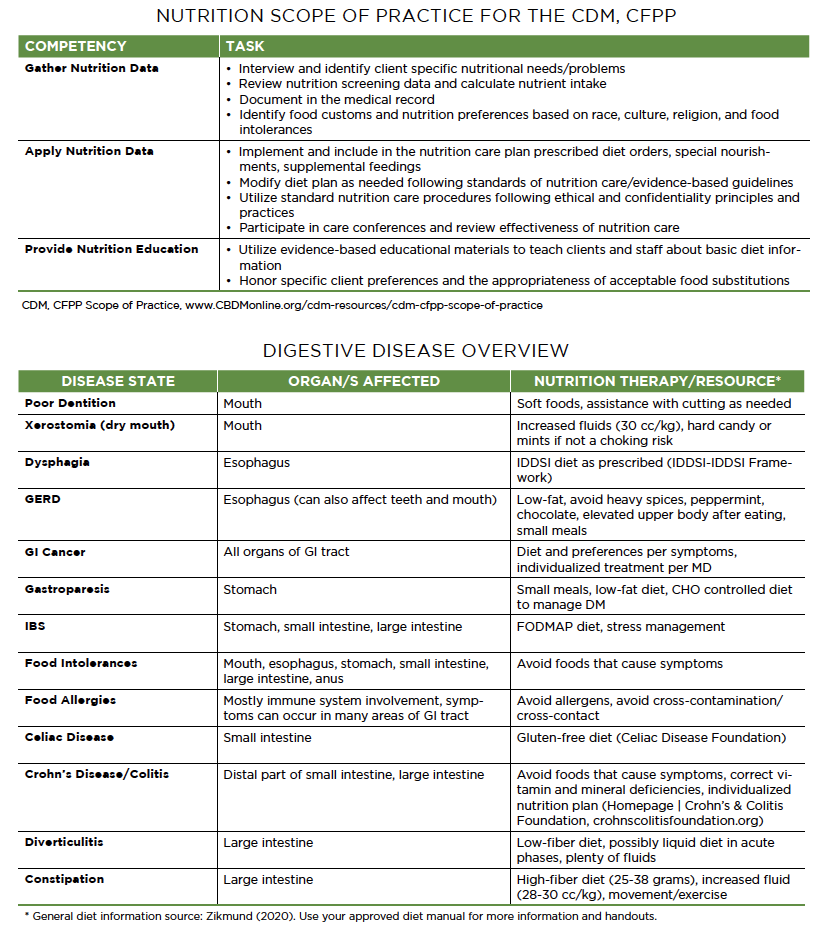
For all aforementioned disease states, individualized medical nutrition therapy with an RDN may be necessary. The CDM, CFPP Scope of Practice for the Nutrition competency can provide guidance as you work with your interdisciplinary team in your role. See figure provided.
SUMMING IT UP
I hope you enjoyed traveling through our digestive system with our lunch and picked up a few bites (or should we say boluses?) along the way!
About the Author
Kristin Klinefelter, MS, RDN, LDN
Kristin Klinefelter is a nutrition consultant in Northern Minnesota, where comfort foods are abundant.